CARDIOCARE CONCEPTS
Case Studies
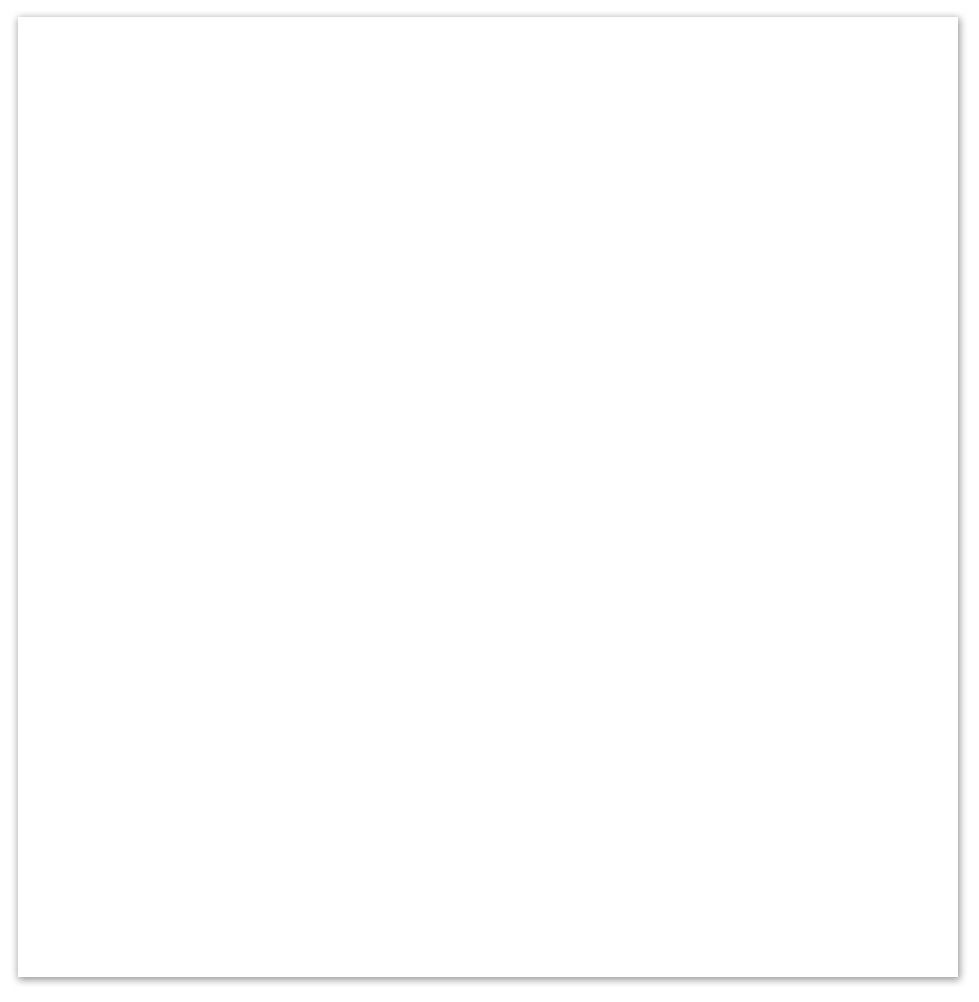
Case 1. Inferior Wall M.I.
Presentation: A 65 y/o male presented with chest and right arm pain. Initial 12 Lead ECG findings show ST segment elevation in leads II, III, and aVF. This is indicative of inferior wall involvement. Reciprocal changes can be seen in the anteroseptal leads in V1, V2, and V3 indicating that there may be posterior wall involvement as well. These findings are consistent with RCA occlusion.
ECG Rhythm: NSR
Diagnosis: This pt was found to have a 100% thrombotic occlusion of the RCA.
Treatment/Prognosis: This pt was immediately sent for cardiac catheterization and the thrombus was removed with stents placed. The pt responded well to treatment and had no further complications.
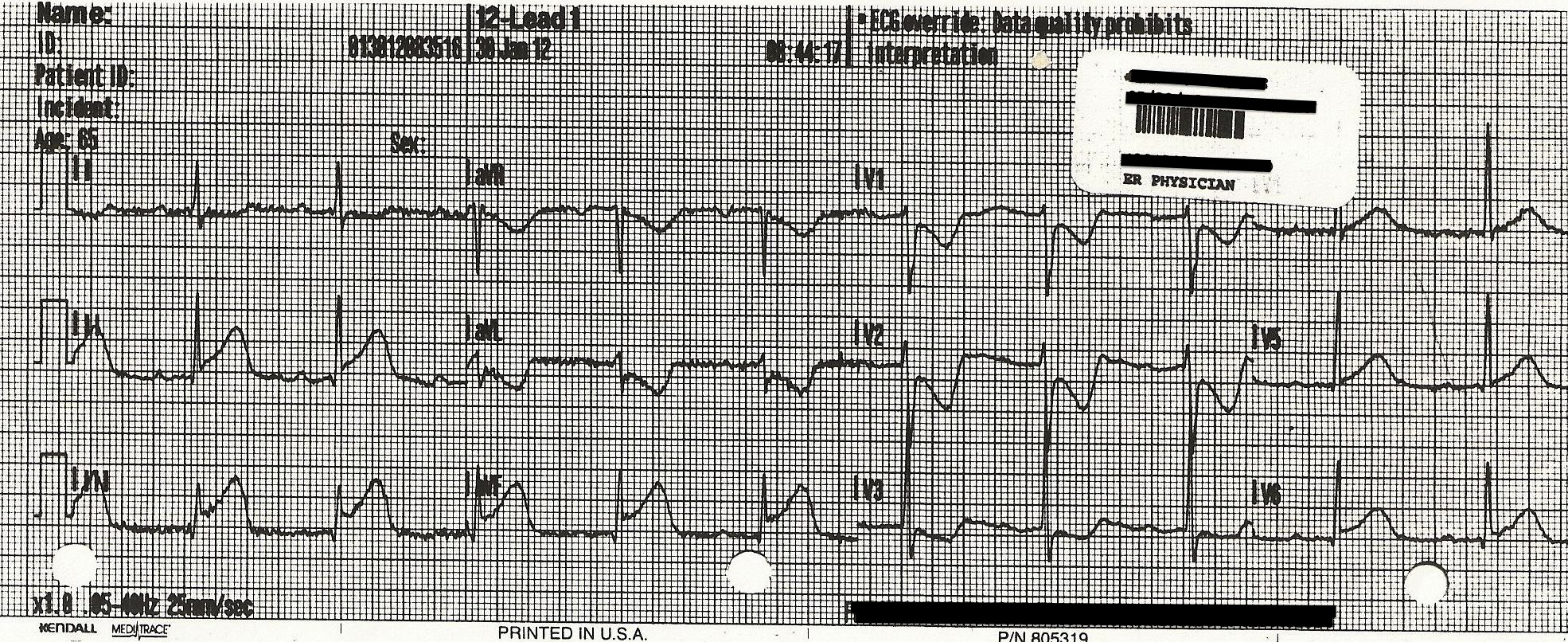
Case 2. Right Ventricular M.I.
Presentation: An 82 y/o female presented as having fallen at home and complaining of weakness. Initial 12 Lead ECG findings show a rhythm with a slow rate. A closer look reveals a complete heart block with junctional escape beats. Also found are ST segment elevation in leads II, III, and aVF. This is indicative of inferior wall myocardial infarction. A V4 Right is performed and is positive for ST segment elevation. This indicates that the right ventricular wall is involved as well.
ECG Rhythm: Complete heart block with junctional escape
Diagnosis: This pt was found to have a 100% thrombotic occlusion of the RCA.
Treatment/Prognosis: Cardiac catheterization and thrombus removed with stents placed. The right ventricle was repurfused and the AV block subsided.
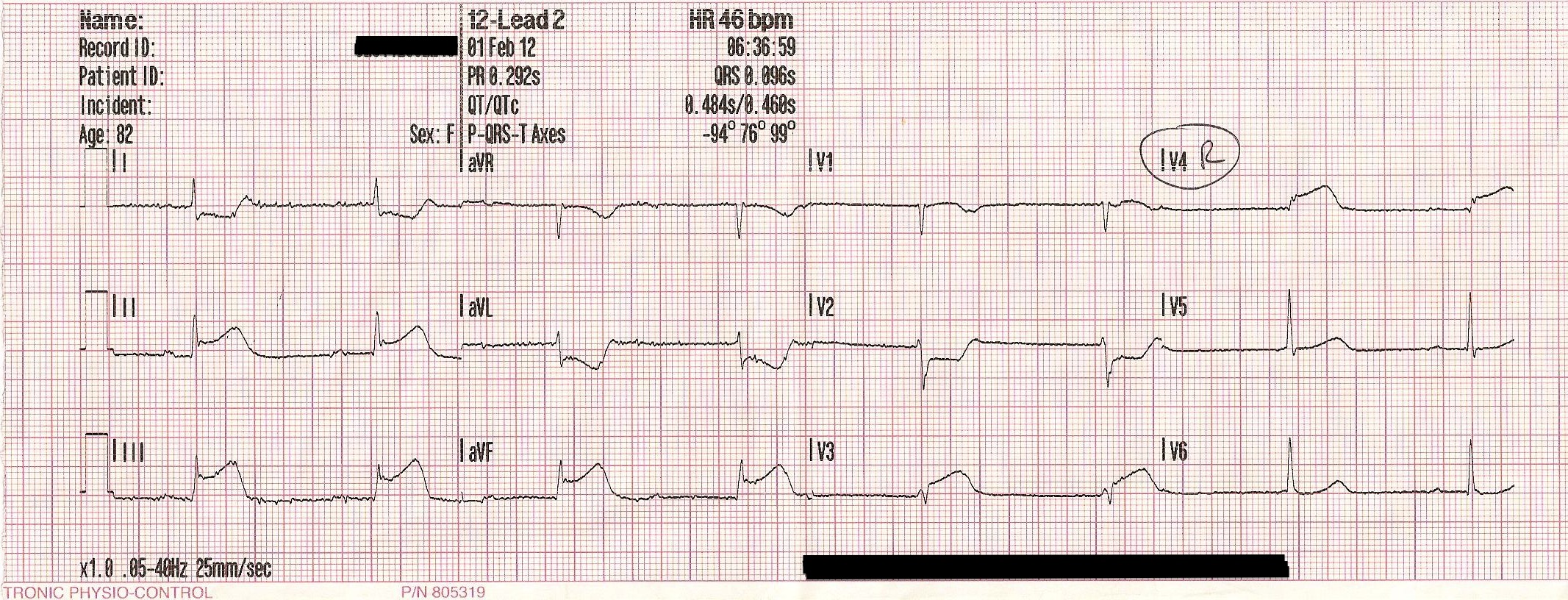
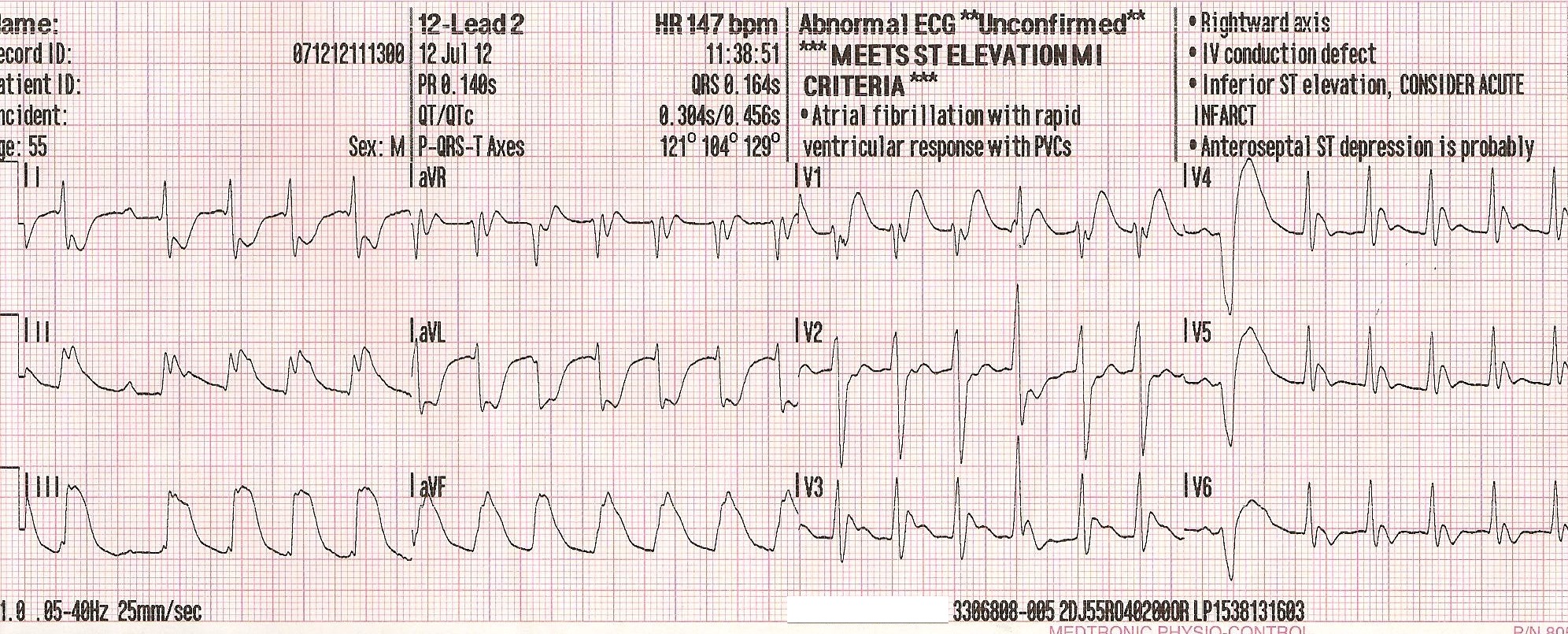
Case 3. Left Main Coronary Artery Occlusion
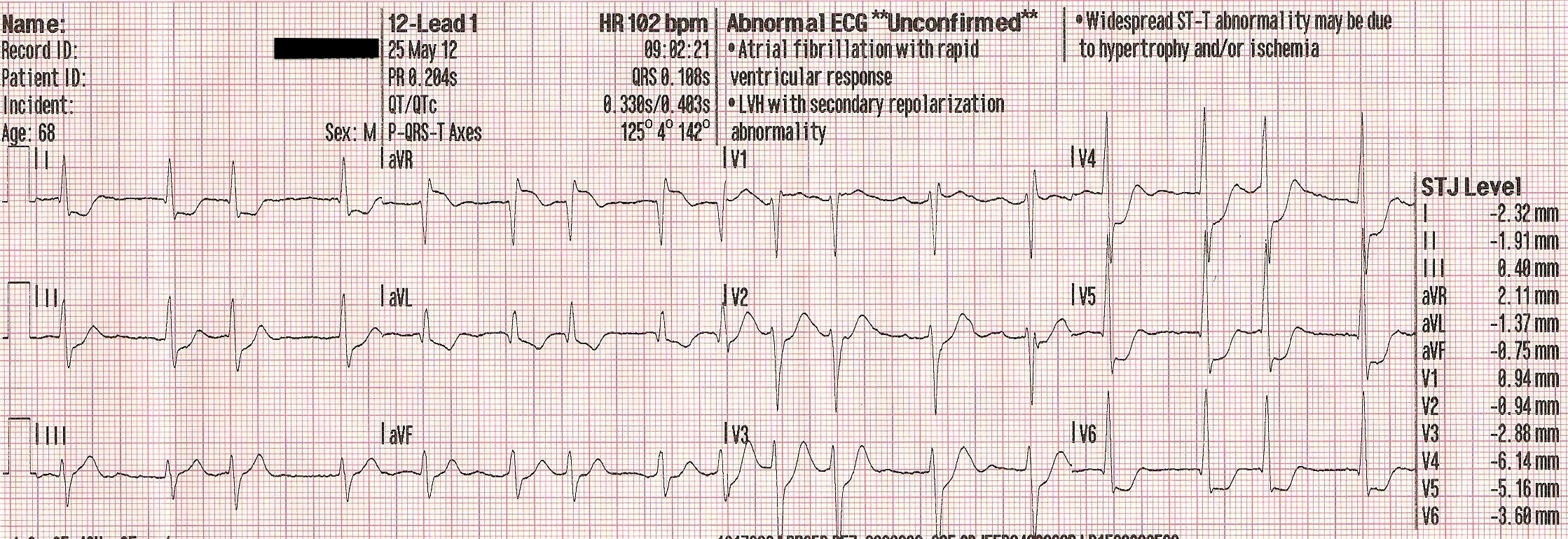
Presentation: A 68 y/o male presented with sudden onset of chest pain followed by cardiac arrest. An AED was deployed and the pt was revived. Initial 12 Lead ECG findings show a somewhat fast rate, which is irregularly irregular. There is ST segment elevation in leads aVR and V1. There is widespread ST segment depression across the anterior and lateral leads including V2 through V6 as well as I and aVL. These findings are consistent with left main coronary artery occlusion.
ECG Rhythm: Rapid atrial fibrillation
Diagnosis: This pt was found to have a left main coronary artery occlusion.
Treatment/Prognosis: This pt was sent to the cardiac cath lab. The pt went into a lethal dysrhythmia and expired shortly after, despite all efforts.
Case 4. Cardiac Arrest - Inferior Wall M.I.
Presentation: A 55 y/o male presented with sudden cardiac arrest at home. Pt was found to be in V-fib. CPR was initiated along with resuscitative efforts including; defibrilation at 360 joules (biphasic), airway management with ET tube intubation and assisted ventilations, epinephrine IV, lidocaine IV. Pt rhythm converted to asystole. CPR continued and further doses of epinephrine IV were administered. Atropine IV was also administered. Pt rhythm converted to an organized with ROSC, and a blood pressure reading. 12 ECG was performed which showed large ST elevations in leads II, III, and aVF indicating an inferior wall M.I.
ECG Rhythm: Sinus rhythm (peri-arrest rhythm)
Diagnosis: This pt was found to have a RCA occlusion with aneurysm.
Treatment/Prognosis: This pt was sent to the cath lab and then immediately for open heart surgery. He was then placed in cardiac ICU and remained on life support.
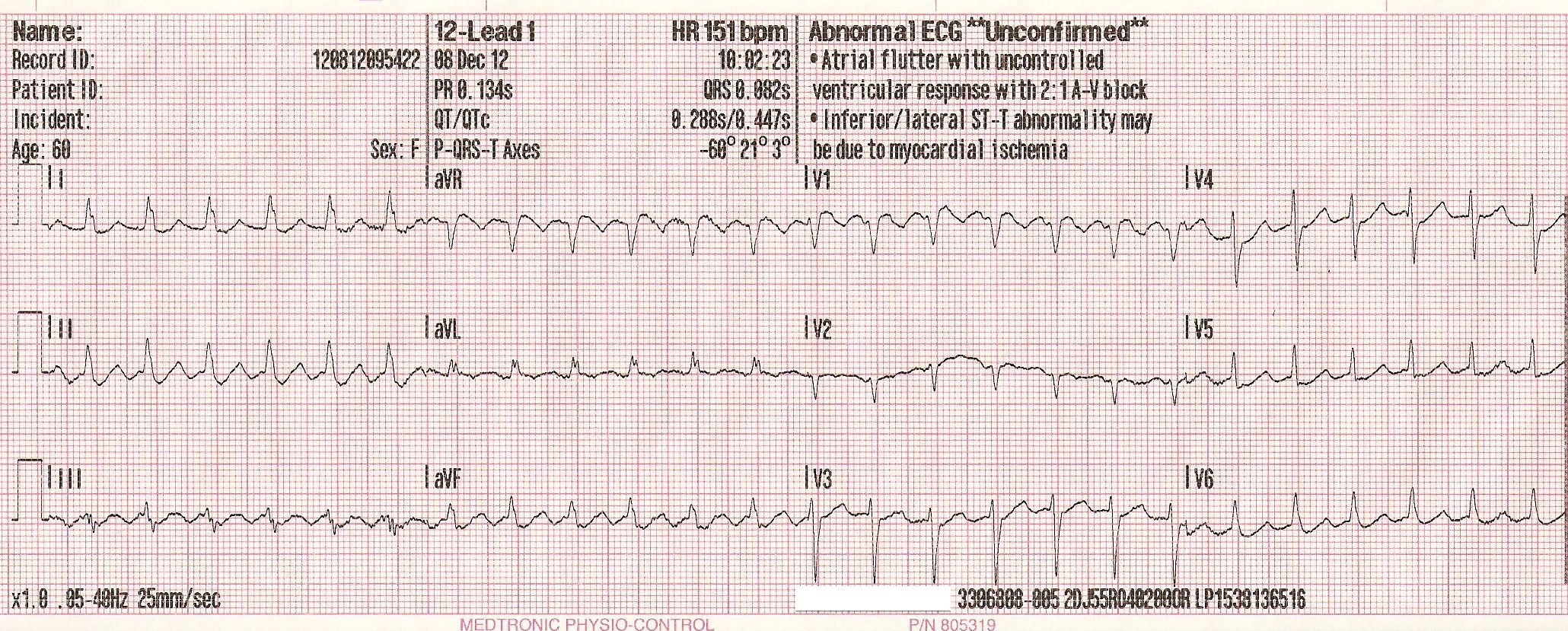
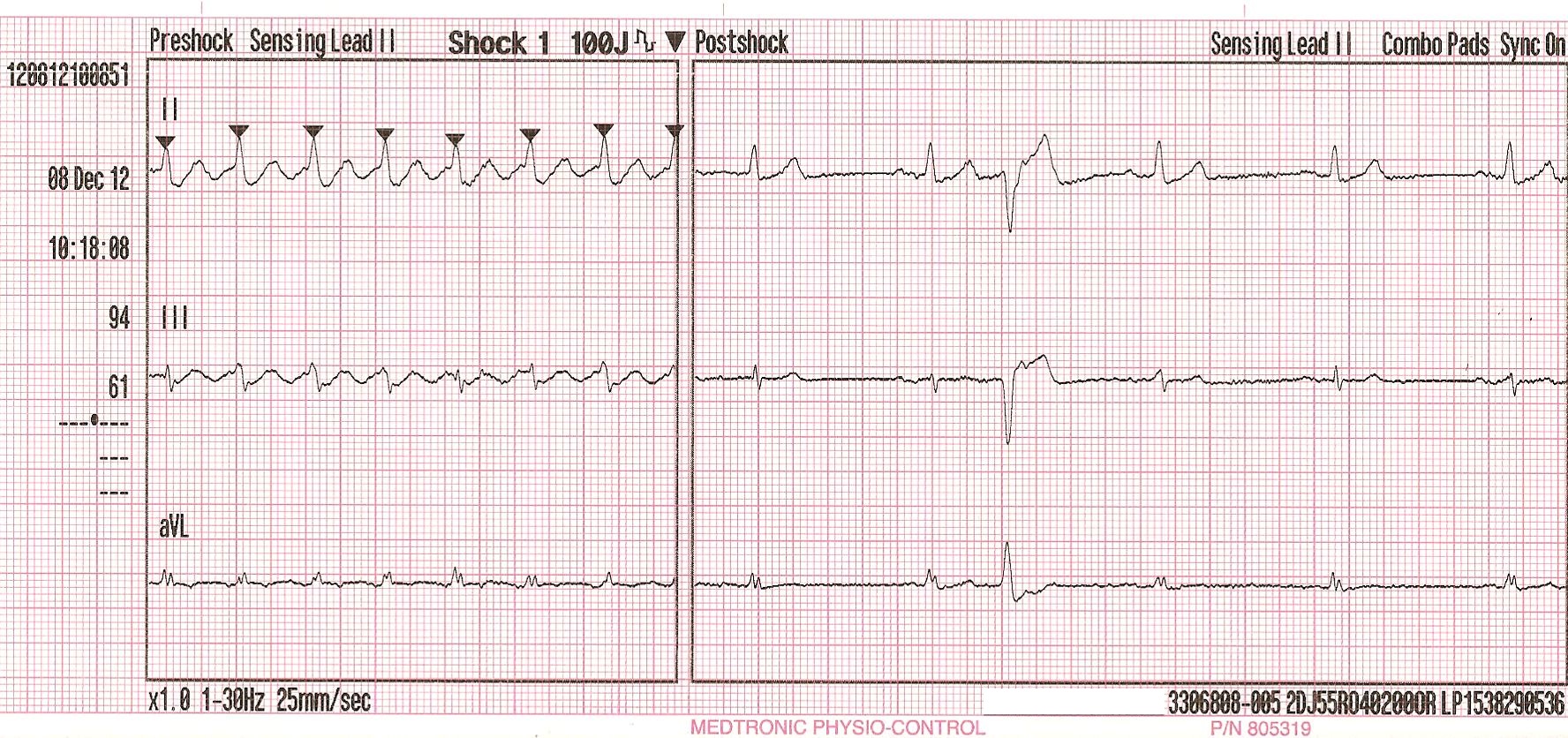
Case 5. Atrial Flutter
Presentation: A 60 y/o female presented with severe weakness and SOB. Initial ECG findings show a narrow complex tachycardia at a rate of 150 bpm. Blood pressure measured 76/40. Pt was pale and diaphoretic. A 12 lead ECG was obtained and showed atrial flutter with a 2:1 conduction ratio. Synchronized cardioversion was performed at 100 joules. Pt's rhythm converted to a sinus rhythm. Signs and symptoms improved including color, blood pressure, and mentation.
ECG Rhythm: Atrial Flutter with 2:1 conduction, converted to NSR
Treatment/Prognosis: This pt was treated in the ER and sent to the EP lab for evaluation.
 | ||||
| ||||
| ||||
| ||||
| ||||
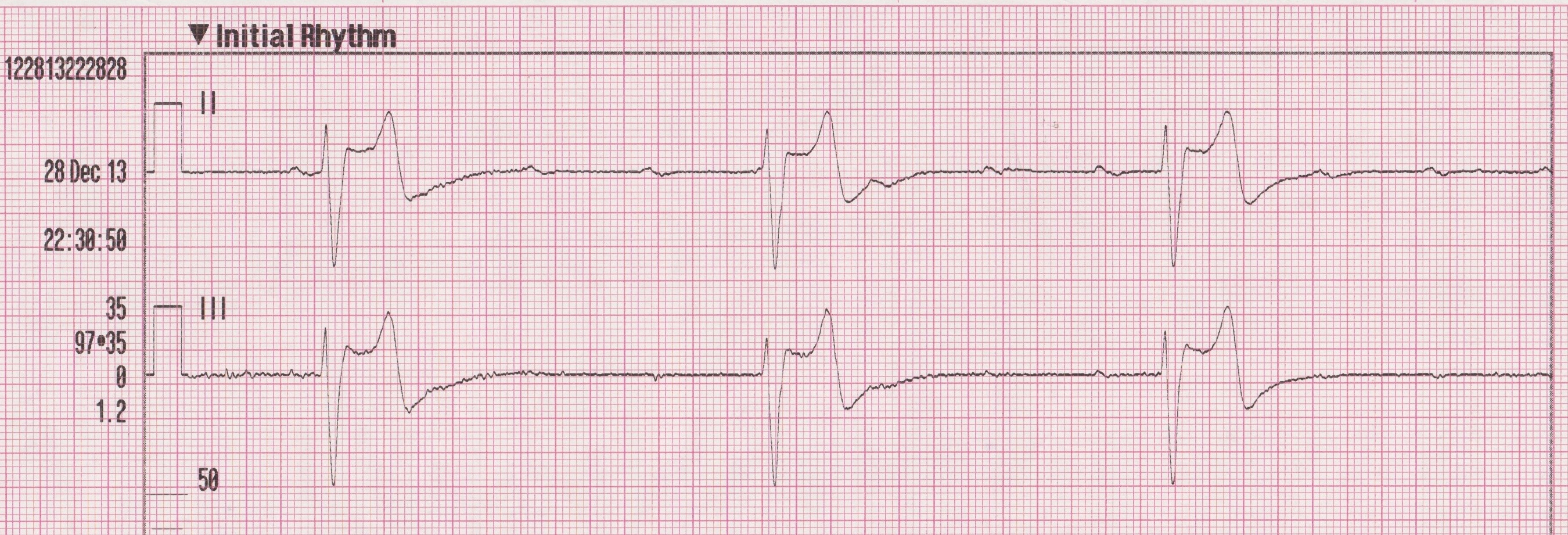
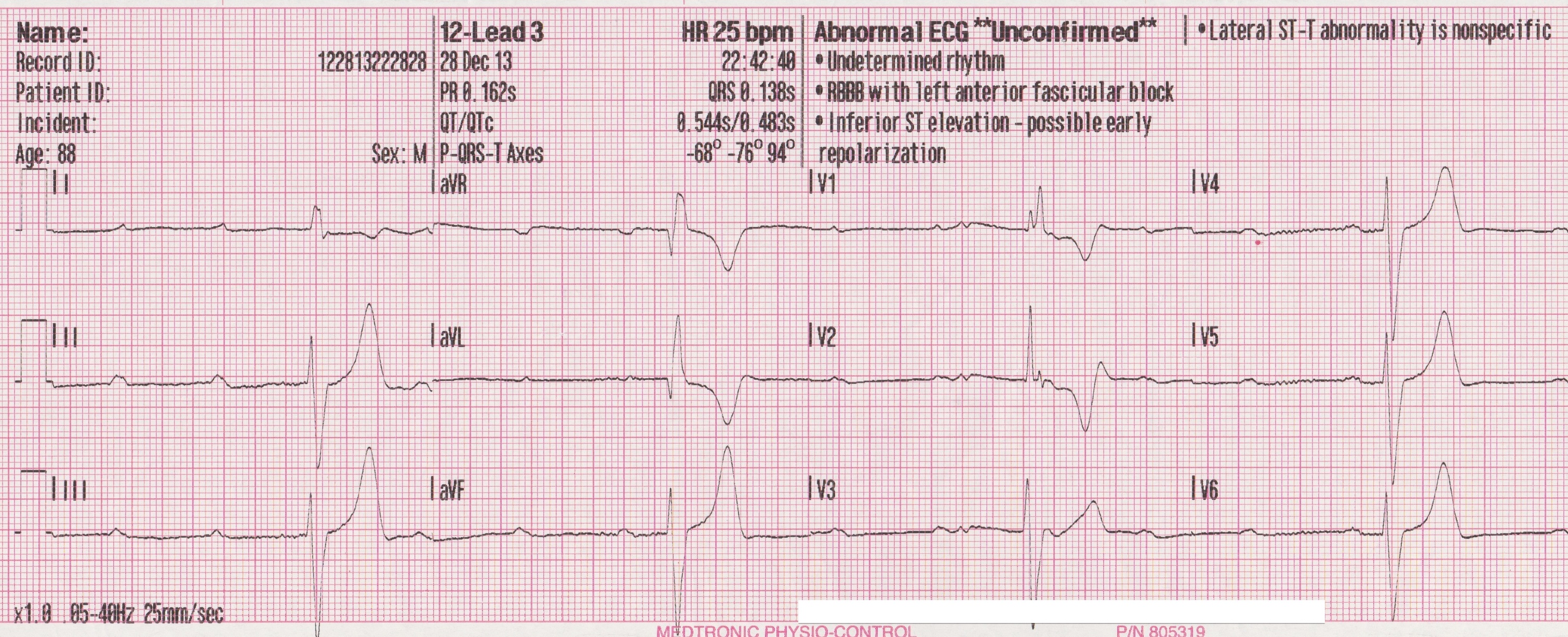
Case 6. Trifascicular Block (CHB) - Bifascicular Block (RBBB / LPFB)
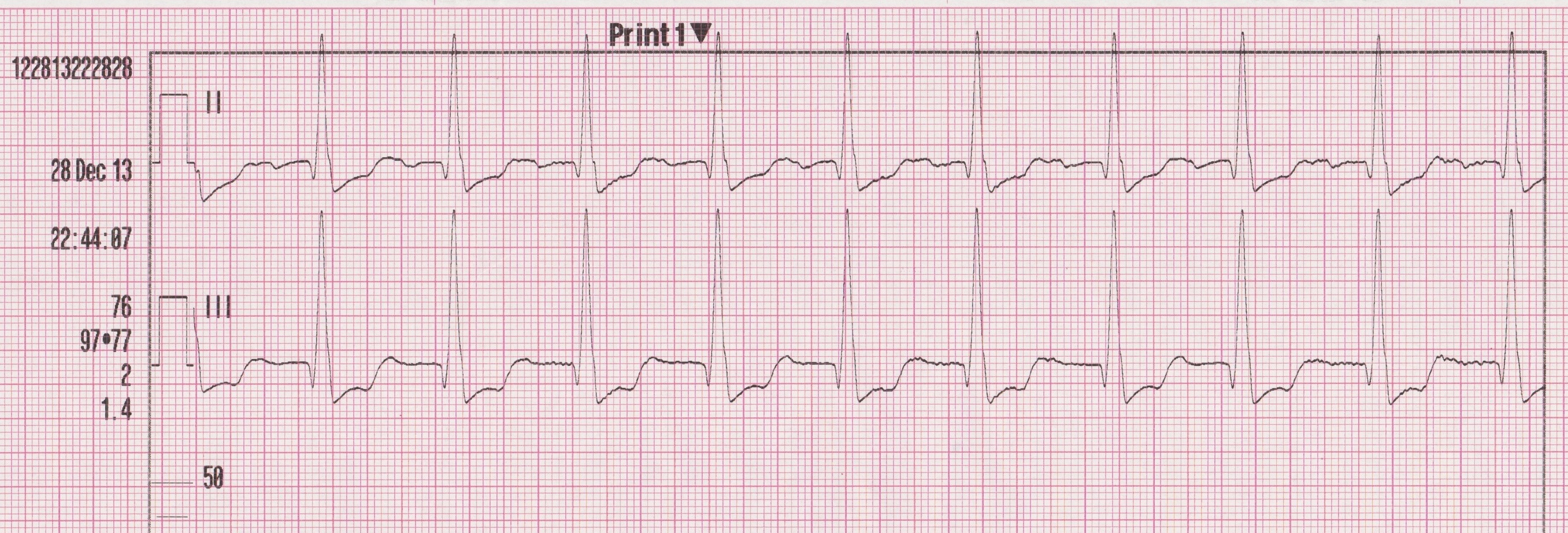
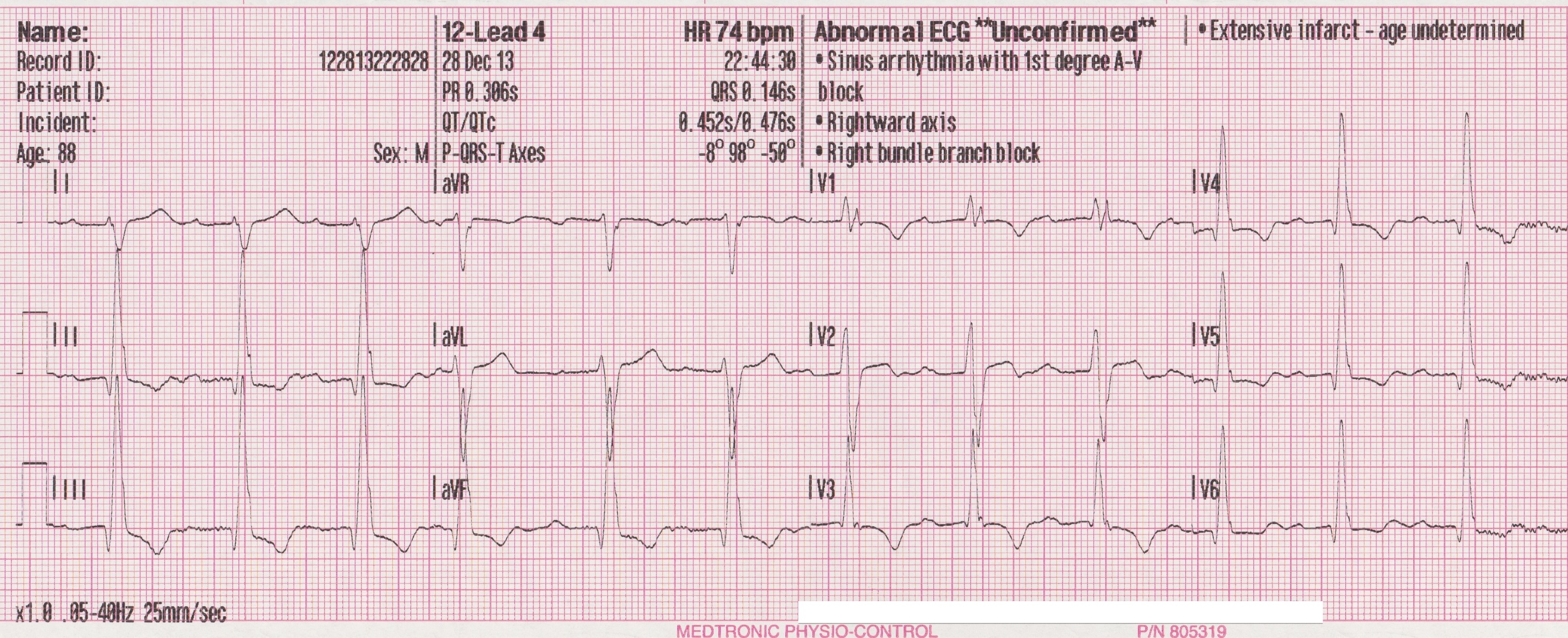
Presentation: An 88 y/o male presented with syncopal episode. Upon EMS arrival, pt was complaining of weakness. Initial ECG rhythm and 12 lead show AV dissociation with likely ventricular escape beats and HR about 25 bpm (CHB). Pt remained hemodynamically stable with a BP of 105/50. During assessment, and prior to any treatment, pt self converted into a sinus rhythm. Post conversion ECG rhythm and 12 lead show a sinus rhythm, first degree AVB with RBBB and HR about 74 BPM. There is also evidence of left posterior fascicular block (LPFB). There is right axis evident in the limb leads as well as prominent S wave in lead I and Q wave in lead III. No LPFB exclusion criteria of RAE or RVH. This would suggest that the initial rhythm was trifascicular block (RBBB/LAFB/LPFB).
ECG Rhythm: Trifascicular block (CHB), followed by first degree AVB with bifascicular block (RBBB/LPFB)
Treatment/Prognosis: This pt was treated in the ER and sent to the EP lab for evaluation. An internal pacemaker was placed.
| ||||
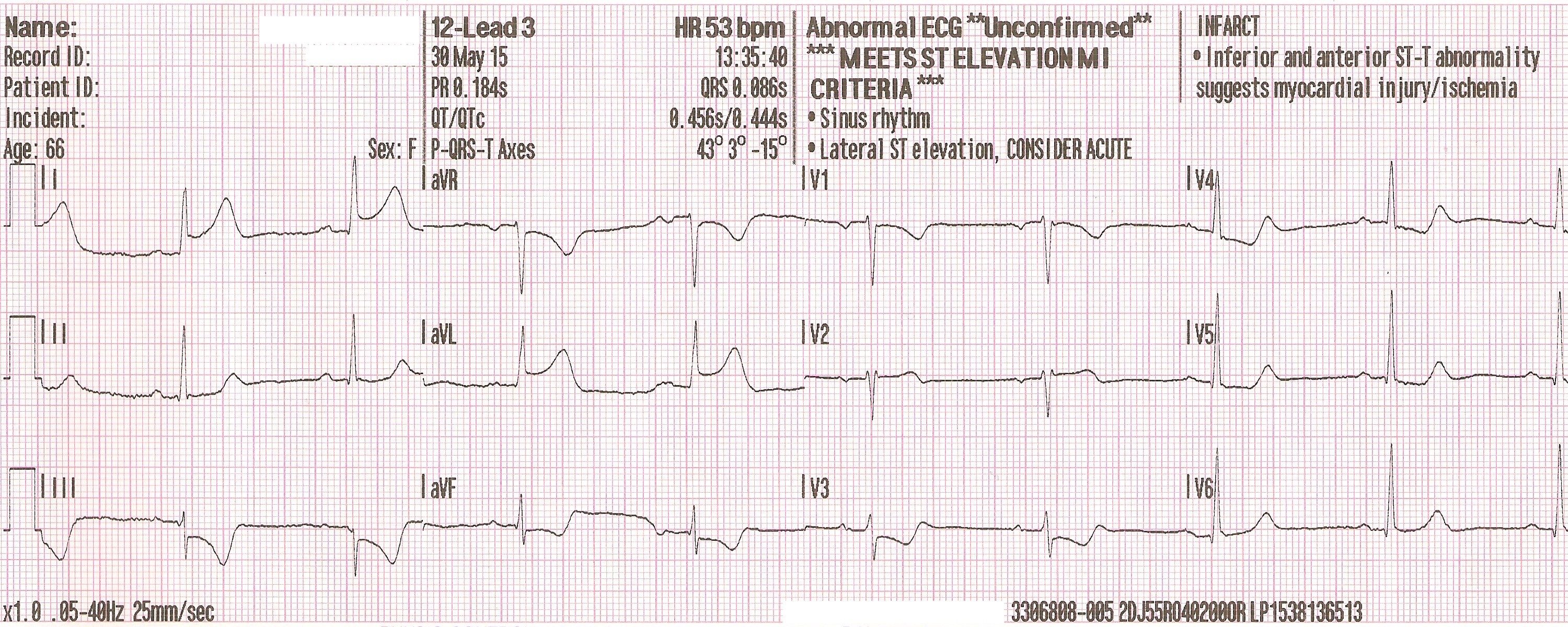
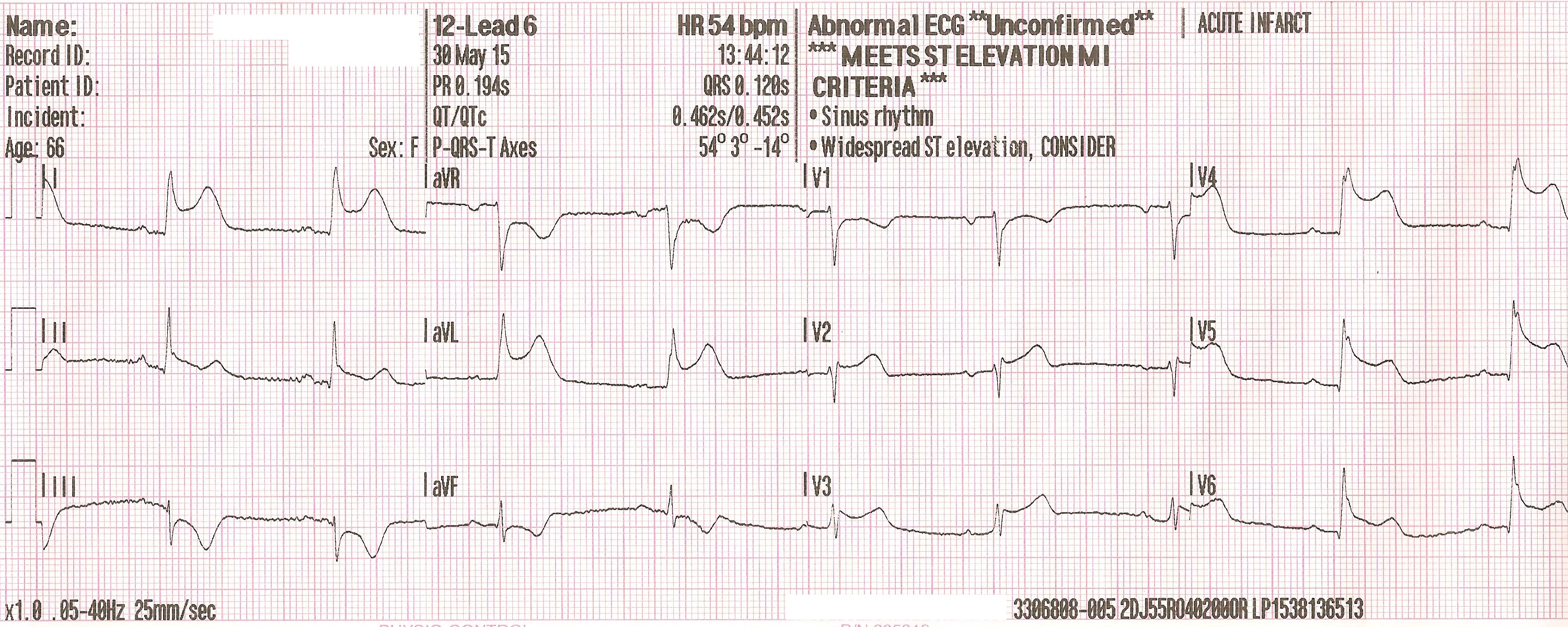
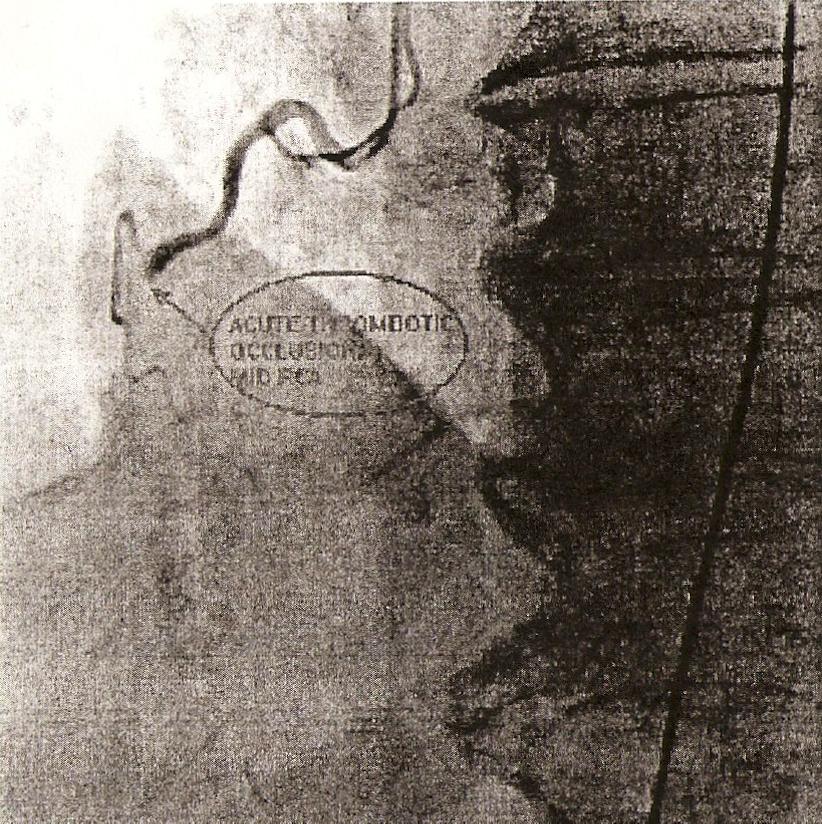
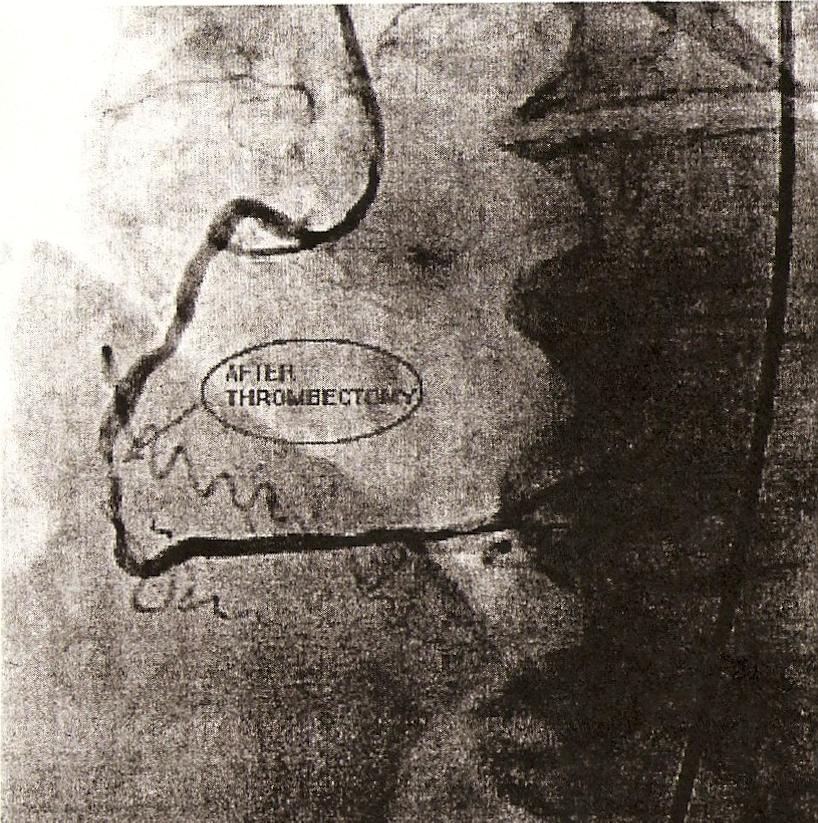
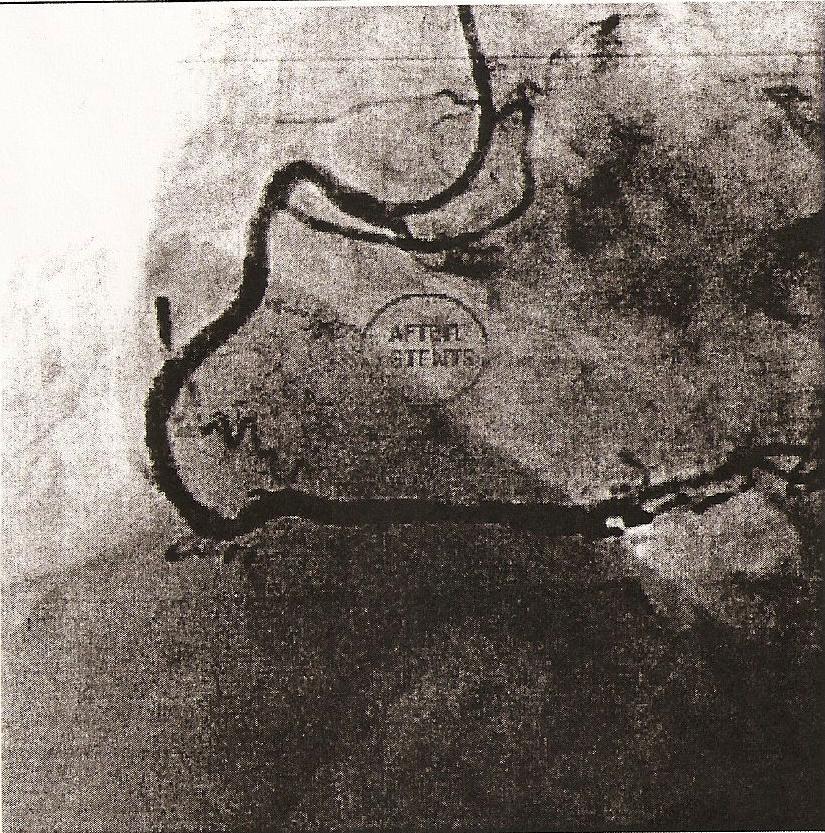
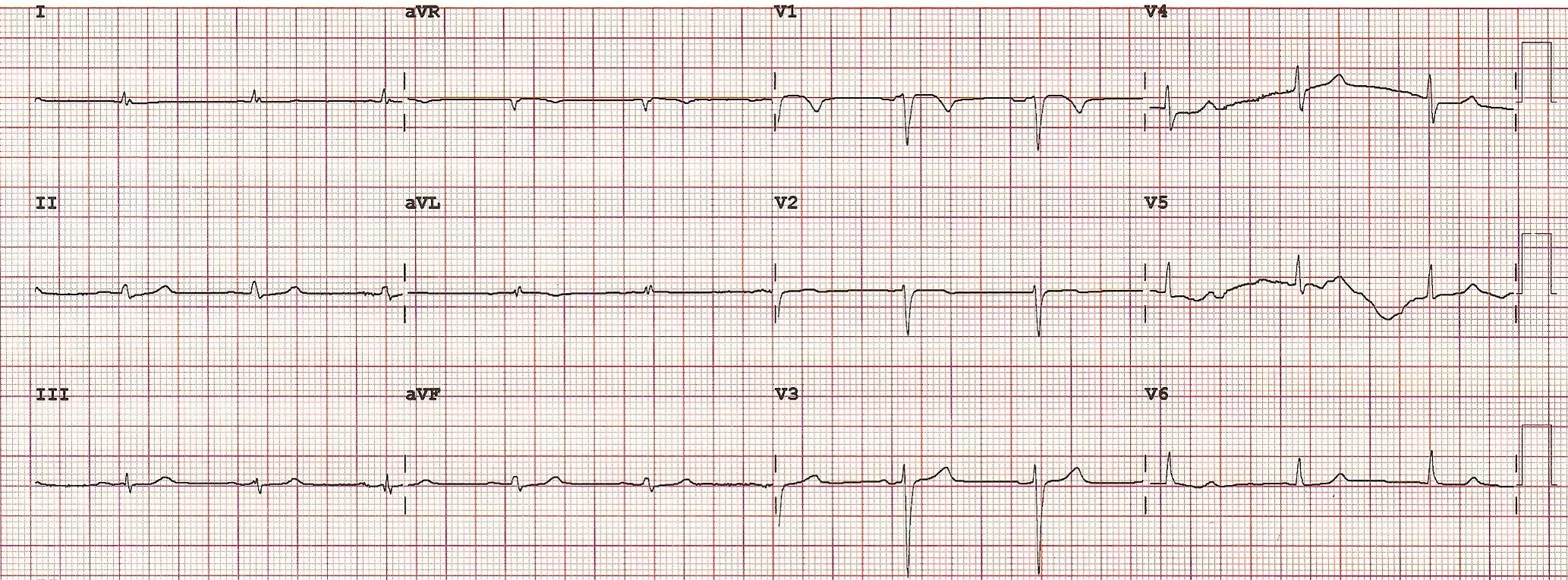
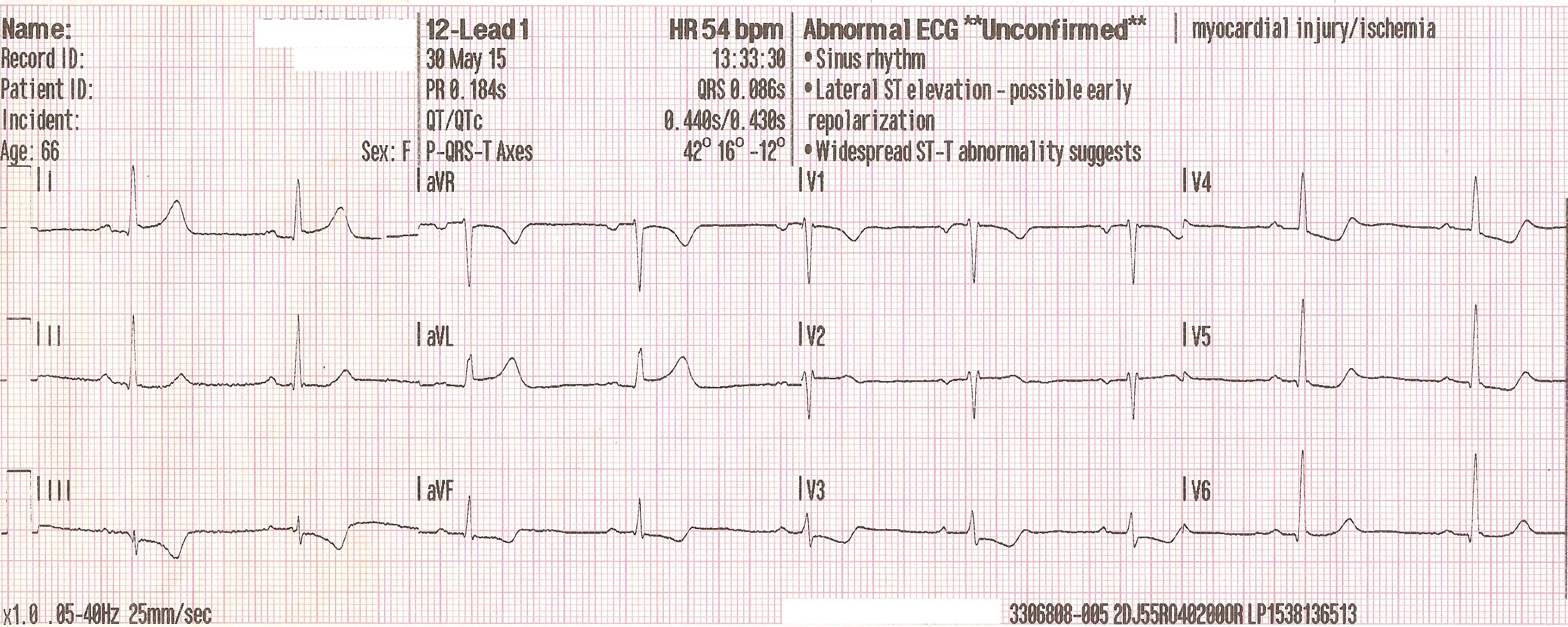
Case 7. STEMI - Anterior Wall MI
Presentation: 66 y/o female presented with sudden onset chest pain after exercising at home. Initial 12 lead ECG showed subtle ST elevations in leads I and aVL as well as depression in lead III and precordial leads. Note the shape of the ST segment elevation. This classic shape along with QRS concordance indicates myocardial ischemia/injury. Note how ST segment elevations increase as MI progresses with subsequent 12 lead ECGs.
| ||||
ECG Rhythm: NSR
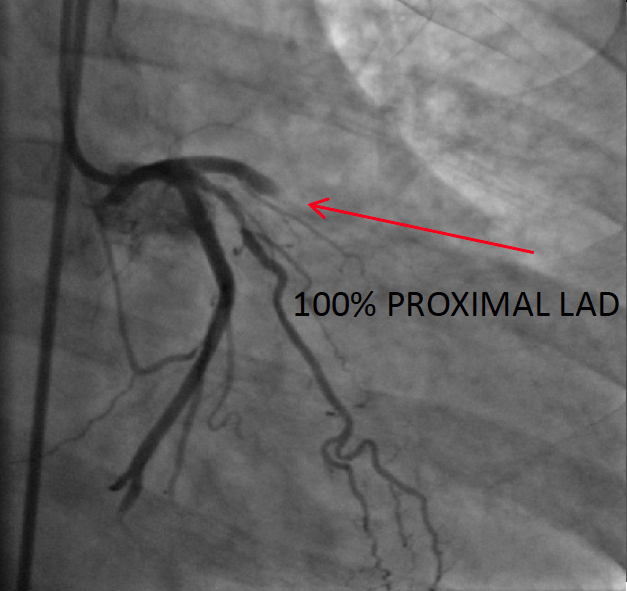
Diagnosis: Anterior Wall MI
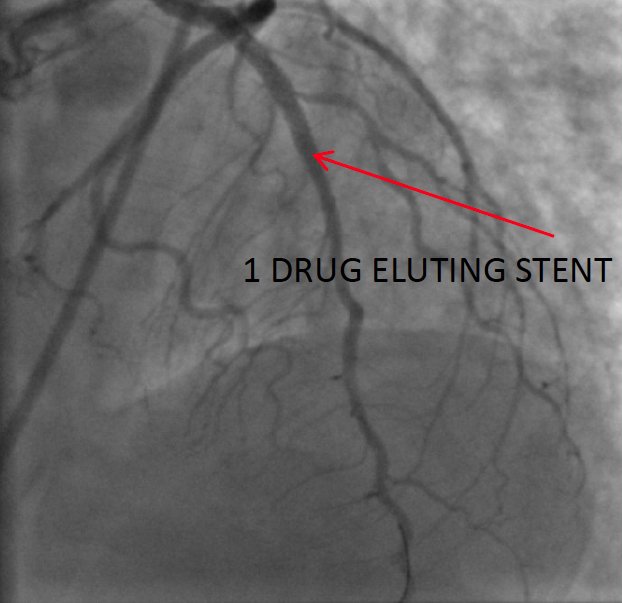
Treatment/prognosis: Pt was transported by EMS to emergency room with STEMI alert protocol initiated. Pt was expedited to cardiac cath lab. A 100% proximal LAD occlusion was identified and a thrombectomy was performed with removal of multiple clots. A drug eluting stent was deployed with reperfusion of the LAD. During the cath, it was evident that she was in cardiogenic shock and a Intra Aortic Balloon Pump was inserted. It was also necessary to defibrillate for V-Tach.